
◆ RESEARCH & KNOWLEDGE HUB
The science, in plain language.
Peptides and GLP-1 medications can sound complicated. They don’t have to be. Here’s how they actually work — explained simply, with visuals, a glossary, and summaries of real studies.
THE BASICS
What are peptides?
In one sentence: Peptides are small chains of amino acids that act like text messages between your cells.
Your body is full of proteins. Peptides are just shorter versions of those — small strings of amino acids (usually 2 to 50 of them) linked together.
Instead of building muscle or tissue like big proteins do, many peptides work as signals. They travel to a cell, attach to it like a key in a lock, and deliver an instruction: release this hormone, repair this tissue, feel full. Some hormones you already know — like insulin — are actually peptides.
Think of it like: a key ring. Each peptide is a differently-shaped key. It only opens the one lock it was cut for — which is why peptides can be so targeted.
How you take a peptide depends on the peptide. Most are given as a small injection under the skin, but some come as capsules, nasal sprays, or creams. Many peptides used for wellness are still being studied and aren’t FDA-approved for those uses — which is why a provider’s guidance matters.
WEIGHT LOSS
Single, dual & triple agonists
In one sentence: Older medications press one “button,” newer ones press two or three — which can mean more weight loss.
An “agonist” is just something that switches a receptor on. Your body has a few different metabolic receptors. How many a medication activates is what separates the generations.

Each extra target is another lever on metabolism and appetite. In studies, adding targets has generally meant more weight loss on average — though more isn’t automatically “better for everyone.” Side effects, cost, and your health history all matter.
*Retatrutide is investigational — it’s still in clinical trials and not FDA-approved. A licensed provider decides what’s appropriate for you.
COMPARISON
Semaglutide vs. tirzepatide
In one sentence: In the first direct comparison, tirzepatide led to more weight loss on average — but both worked well.
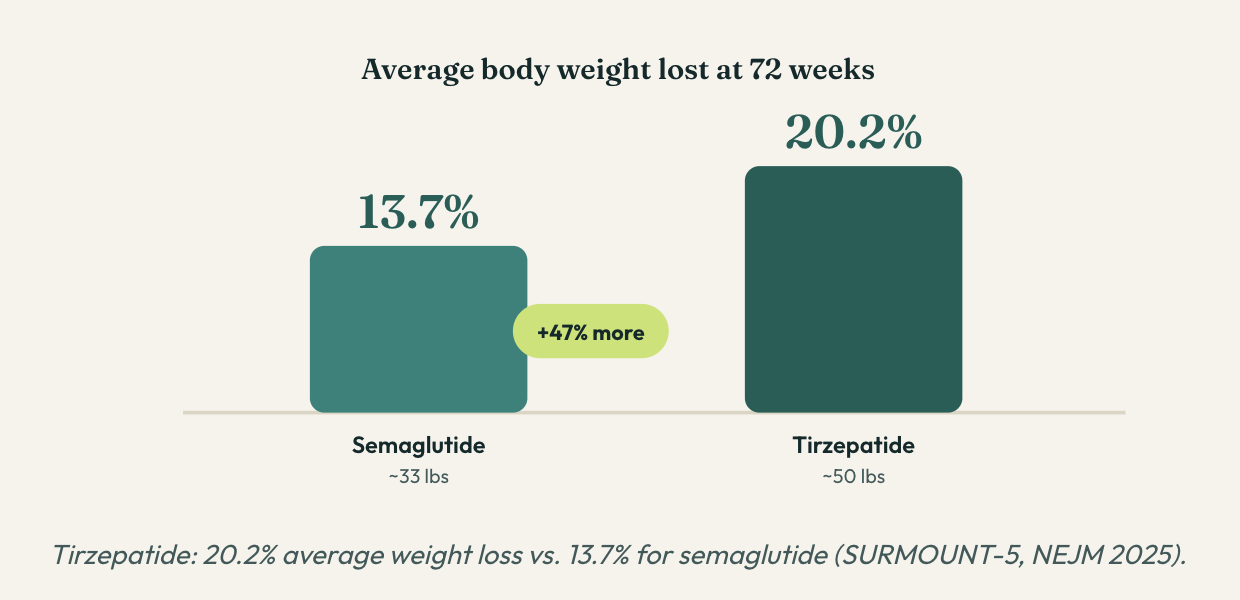
About 1 in 3 people on tirzepatide lost a quarter of their body weight or more, versus about 1 in 6 on semaglutide. Side effects differed too: semaglutide leaned toward nausea, tirzepatide toward diarrhea — mostly during the early dose-increase phase.
The takeaway: tirzepatide won on average, but “best on average” isn’t the same as “best for you.” Both are effective tools, and the right choice depends on how your body responds, tolerability, and cost.
RECOVERY
Recovery & repair peptides
In one sentence: Peptides like BPC-157 look promising for healing in early research, but most evidence is still from animal studies.
BPC-157, TB-500, and GHK-Cu are the peptides people talk about for recovery. BPC-157 is the most studied. Researchers think it helps the body’s natural repair crew work faster.

This is especially interesting for tendons and ligaments, which normally heal slowly because they get little blood flow. A 2025 review of 36 studies found BPC-157 consistently improved healing outcomes across these models.
The honest part: almost all of that research is in animals, not people. Human studies are still rare, there’s no official dosing standard, BPC-157 isn’t FDA-approved, and it’s banned in pro sports. Promising — but early.
LONGEVITY
Longevity & NAD+
In one sentence: NAD+ helps your cells make energy, it drops as you age, and topping it up is a hot research area — with results still coming in.
Every cell has tiny power plants called mitochondria. To make energy, they rely on a helper molecule: NAD+. As we get older, NAD+ levels fall — and scientists wonder if that decline is part of why we feel the effects of aging.
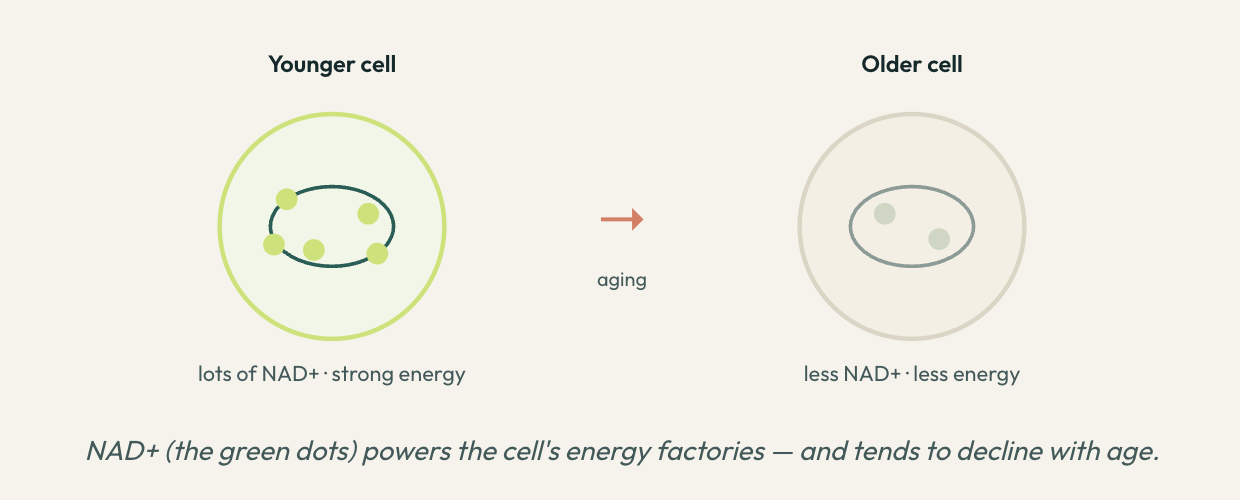
Where the science stands: NAD+ boosters reliably raise NAD+ levels and are generally well tolerated. But proof that they deliver big anti-aging or energy benefits in humans is still mixed. It’s a promising, active area — not a settled “fountain of youth.”
These guides are simplified for general education and aren’t medical advice. Always talk to a licensed provider before starting any therapy.
Plain-English glossary
Every term you’ll run into, explained without the jargon.
Studies & findings
Real research, summarized in everyday terms. Numbers come from published studies — but every person is different, so treat these as background, not promises.
HEAD-TO-HEAD · 2025
20.2%
SURMOUNT-5 · New England Journal of Medicine, 2025
TRIPLE AGONIST · 2025
24.2%
Jastreboff et al. · NEJM, 2023 (Phase 2)
PHASE 3 · 2026
16.8%
In people with type 2 diabetes, the 12 mg dose led to an average 36.6 lb (16.8%) loss at 40 weeks, with no weight-loss plateau seen through the study.
Eli Lilly topline results · March 2026
RECOVERY · PRECLINICAL
36
Systematic review · HSS Journal, 2025
SKIN · CLINICAL
55.8%
An 8-week randomized, double-blind trial of a GHK-Cu serum reported a 55.8% reduction in wrinkle volume and 32.8% in wrinkle depth versus control.
Controlled clinical trial (Badenhorst et al.)
LONGEVITY
113
PRISMA systematic review · 2026